
Indexed In
- Open J Gate
- Genamics JournalSeek
- Academic Keys
- JournalTOCs
- China National Knowledge Infrastructure (CNKI)
- Ulrich's Periodicals Directory
- RefSeek
- Hamdard University
- EBSCO A-Z
- Directory of Abstract Indexing for Journals
- OCLC- WorldCat
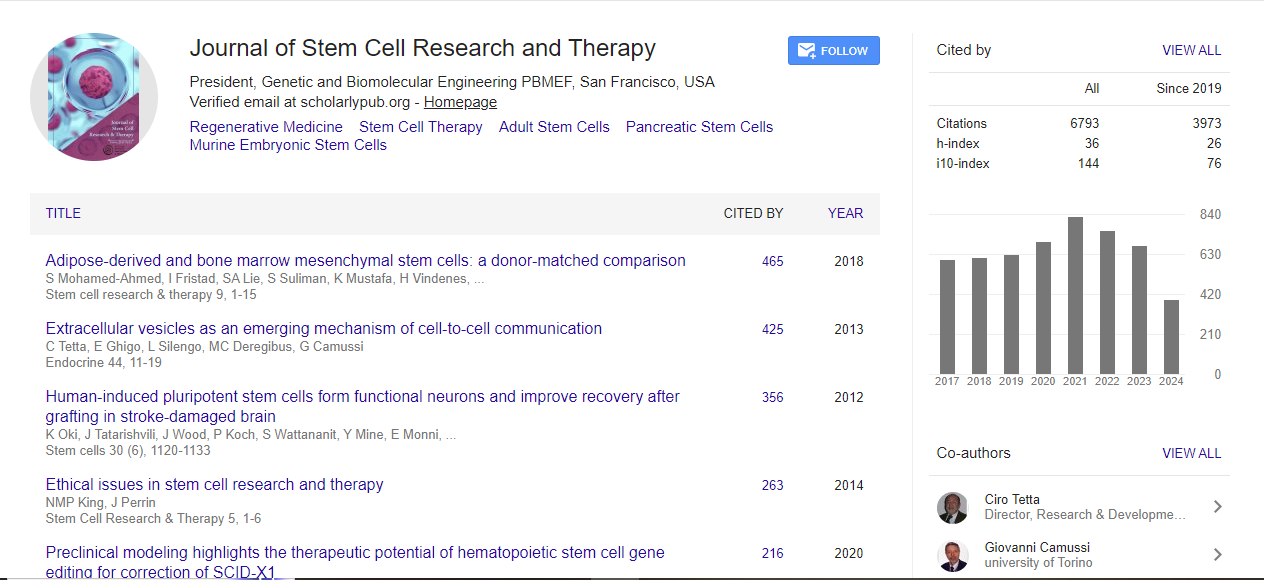
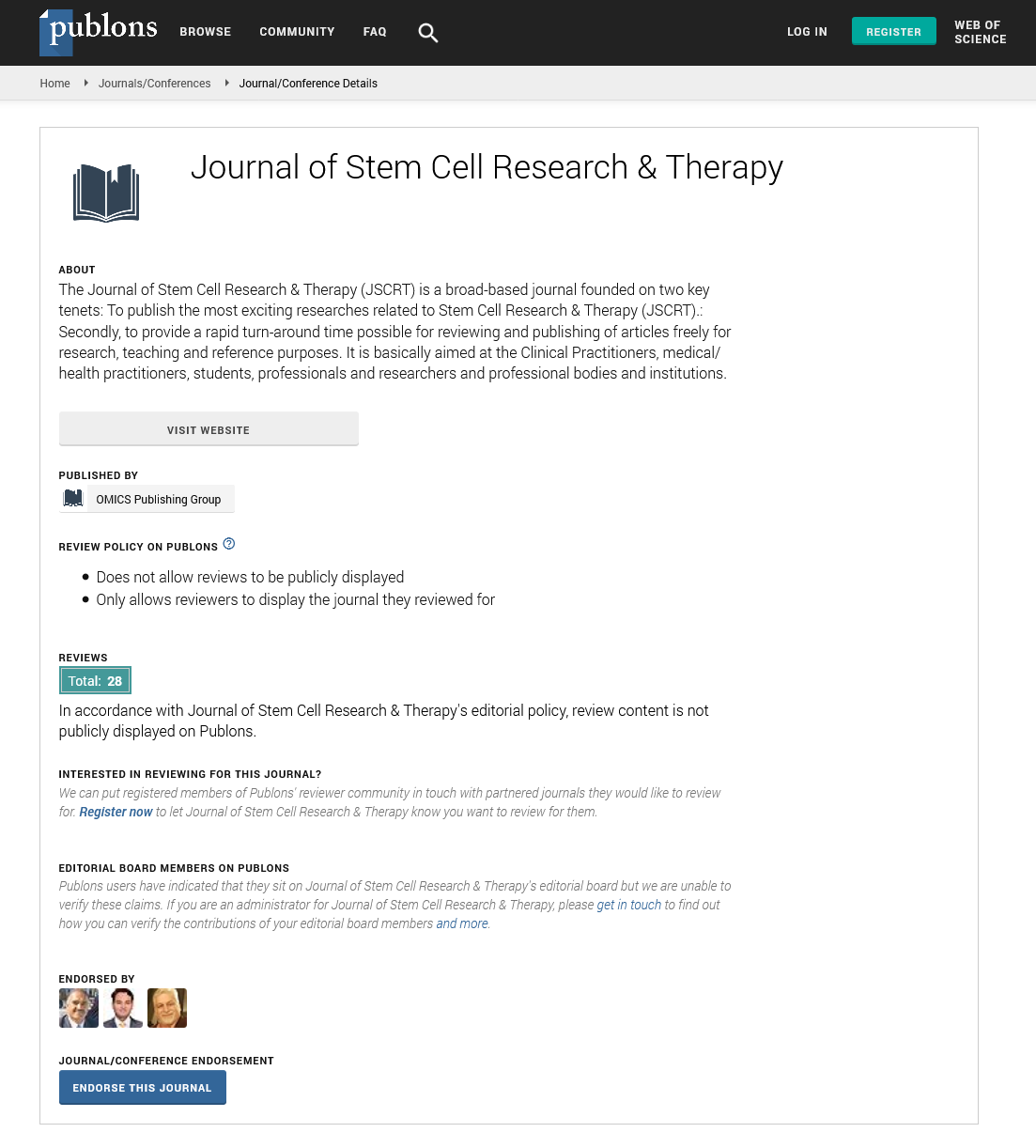
- Publons
- Geneva Foundation for Medical Education and Research
- Euro Pub
- Google Scholar
Useful Links
Share This Page
Journal Flyer

Open Access Journals
- Agri and Aquaculture
- Biochemistry
- Bioinformatics & Systems Biology
- Business & Management
- Chemistry
- Clinical Sciences
- Engineering
- Food & Nutrition
- General Science
- Genetics & Molecular Biology
- Immunology & Microbiology
- Medical Sciences
- Neuroscience & Psychology
- Nursing & Health Care
- Pharmaceutical Sciences
Intracoronary infusion of a very primitive population of mesenchymal stem cells in acute myocardial infarction: A randomized, double-blind, placebo controlled, multicenter trial
3rd International Conference and Exhibition on Cell & Gene Therapy
October 27-29, 2014 Embassy Suites Las Vegas, USA
Lian Ru Gao
Scientific Tracks Abstracts: J Stem Cell Res Ther
Abstract:
Context: The use of adult stem cells is limited by the quality and quantity of host stem cells. Wharton?s jelly?derived mesenchymal stem cells (WJMSCs), a very primitive population, may integrate into ischemic cardiac tissues and significantly improve heart function in preclinical models. Objective: To assess the safety and efficacy of intracoronary infusions of WJMSCs in patients with ST-elevation acute myocardial infarction (AMI) in a randomized, double-blind, placebo-controlled study. Design, Setting, and Patients: Subjects with AMI (n=160) were screened and 116 eligible patients were randomly assigned to receive an intracoronary infusion of WJMSCs or placebo into the infarcted artery 5-7 days after successful reperfusion therapy at 11 hospitals in China. Main Outcome Measures For the primary endpoint of safety: The incidence of adverse events (AEs) within 12 months was monitored and quantified. For the endpoint of efficacy: the absolute change in global left ventricular ejection fraction (LVEF) from baseline to 12 months, myocardial viability and perfusion in the infarcted region from baseline to 4 months were measured using two-dimensional echocardiography, F-18-fluorodeoxyglucose positron emission computed tomography (F-18-FDGPET) and 99mTc-sestamibi single-photon emission computed tomography (99mTc-SPECT), respectively. Results: During 12 months follow-up, adverse event rates and laboratory tests including tumor, immune, renal, hepatic, and hematologic indexes were not different for patients receiving WJMSCs or placebo. The absolute improvements in the myocardial viability and perfusion within the infarcted territory at the 4-month follow-up in patients receiving WJMSCs (6.9?0.6%, 95% CI 5.7-8.2 and 7.1?0.8%, 5.4-8.8, respectively) were significantly greater than those in patients receiving placebo (3.3?0.7%,1.8-4.7, P<0.0001, and 3.9?0.6%, 2.8-5.0, P=0.002, respectively). The absolute increase in LVEF at 12 months in the WJMSC group was significantly greater than that in the placebo group (6.7?0.8%, 5.1-8.3 vs. 3.5?0.8%, 1.9-5.0, P=0.004). The LV end-systolic volumes at 12 months was significantly decreased from those at baseline in the WJMSC group (P=0.0002), whereas no significant changes were observed in the placebo group. Conclusion: Intracoronary infusion of WJMSCs is safe and effective in patients with AMI, providing clinically relevant therapy within a favorable time window and at an effective dose. This study encourages additional clinical trials to determine whether WJMSCs may serve as a novel allogeneic source for cardiac stem cell-based therapy.