
Indexed In
- Open J Gate
- Genamics JournalSeek
- ResearchBible
- Electronic Journals Library
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- SWB online catalog
- Virtual Library of Biology (vifabio)
- Publons
- Euro Pub
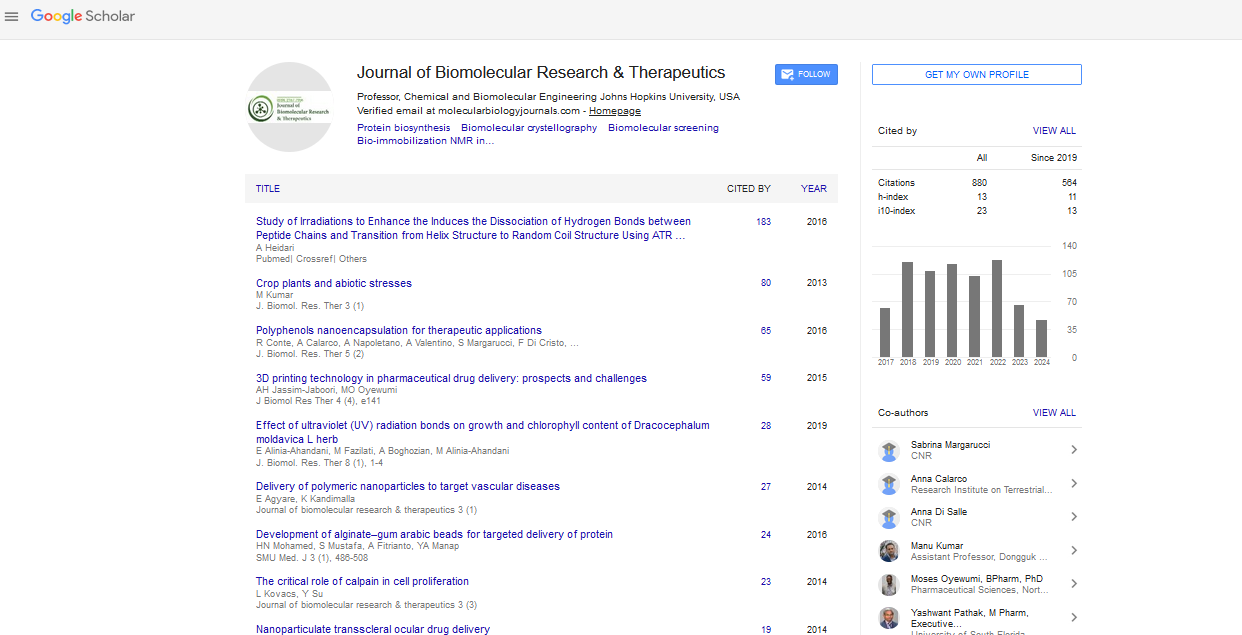
- Google Scholar
Useful Links
Share This Page
Journal Flyer

Open Access Journals
- Agri and Aquaculture
- Biochemistry
- Bioinformatics & Systems Biology
- Business & Management
- Chemistry
- Clinical Sciences
- Engineering
- Food & Nutrition
- General Science
- Genetics & Molecular Biology
- Immunology & Microbiology
- Medical Sciences
- Neuroscience & Psychology
- Nursing & Health Care
- Pharmaceutical Sciences
Commentary - (2023) Volume 12, Issue 2
Therapy and History of Sarcomatoid in Renal Cell Carcinoma
Zhu Kong*Received: 03-Feb-2023, Manuscript No. BOM-23-20102; Editor assigned: 06-Feb-2023, Pre QC No. BOM-23-20102(PQ); Reviewed: 21-Feb-2023, QC No. BOM-23-20102; Revised: 28-Feb-2023, Manuscript No. BOM-23-20102(R); Published: 07-Mar-2023, DOI: 10.35248/2167-7956.23.12.263
Description
Sarcomatoid differentiation is a rare characteristic that can occur in the majority of tumor types of Renal Cell Carcinomas (RCCs) and is associated with a very bad prognosis. Historically, standard treatments for sarcomatoid RCCs (sRCCs) have been ineffective with median survival ranging. Despite being identified in 1968 the mechanisms underlying sarcomatoid dedifferentiation remain poorly understood and clinicians and patients have limited information and treatment options. When detected early, surgical surgery remains the therapy of choice. Preoperative detection with routine imaging or biopsy, on the other hand, is unreliable, and the majority of patients present with advanced illness and systemic symptoms. Sarcomatoid dedifferentiation is an uncommon change that can occur in various RCC histological subtypes and predicts a very bad prognosis. Sarcomatoid RCCs (sRCCs) are RCCs that have undergone sarcomatoid dedifferentiation and patients with sRCCs frequently present with advanced or metastatic illness. To distinguish these variants from renal soft-tissue sarcoma and normal RCCs, the term carcinosarcoma of the kidney is a kind of renal cancer that resembled a sarcoma and had pleomorphic spindle-cell and giant-cell morphology. sarcomatoid RCC appears to be a complicated tumour of an entirely different type and has the appearance of a double neoplasm one component of which is cancer.
Diagnostic sample of the main tumour is advised because the well-differentiated epithelial component and the dedifferentiated sarcomatoid component may only be leading to underdiagnoses. Immunohistochemical markers such as markers of renal histogenesis can aid in resolving this diagnostic quandary. In the absence of a low-grade epithelial component such markers are useful because a tumor with spindled morphology has a broad differential diagnosis which includes sarcomatoid invasive lobular carcinoma, angiomyolipoma, nondividing liposarcoma, sarcomatoid adrenocortical squamous cell and myofibroblasts neoplasms such as single fibrous tumour cells and synovial. Since the early 2000s the usage of percutaneous renal biopsy for suspected tumours has increased. Although percutaneous biopsies have shown good concordance with histological classification during nephrectomy, detecting the presence of sarcomatoid trans differentiation can be difficult. The volume of tissue retrieved by core biopsy as well as the number and spatial distribution of biopsy cores limit the ability to identify sarcomatoid characteristics. Sarcomatoid characteristics are frequently found in 50% of sRCC tumours which are typically big heterogeneous masses. As a result preoperative biopsies have a low sensitivity for sRCCs and are likely non-diagnostic for these traits. Multi-quadrant biopsies have demonstrated increased sensitivity in the diagnosis of sRCCs66. In one study standard single biopsy was compared to multi-quadrant biopsy (biopsies from at least four independent solid enhancing regions. However, because the majority of sRCC patients come with advanced or metastatic disease the usefulness of nephrectomy is debatable. According to a 2009 study based on cytokines chronic therapy patients with metastatic sRCCs should first have a trial of systemic therapy and then be offered chemo radiotherapy nephrectomy if a response is evident. Immune checkpoint inhibitors have made the most progress in the treatment of sRCCs when compared to other systemic treatments. Tumors with constitutive or high levels of adaptive PDL1 expression patterns as well as high amounts of tumor-infiltrating lymphocytes are more likely to react to immune.
Citation: Kong Z (2023) Therapy and History of Sarcomatoid in Renal Cell Carcinoma. J Biol Res Ther. 12:258.
Copyright: © 2023 Kong Z. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.